Toxic or ischemic injury
Acetaminophen overdose, shock liver, severe heat injury, mushroom poisoning, and some drugs can injure many liver cells quickly.
Patient guide + clinician detail
Liver failure is not one diagnosis. It is a dangerous final pathway reached by different problems: toxins, infections, alcohol, metabolic fatty liver disease, autoimmune disease, inherited disorders, blocked blood flow, shock, pregnancy complications, and advanced scarring.
First principle
Think of the liver as the body's chemical processing plant. It clears toxins, helps blood clot, stores energy, handles many medicines, and makes bile for digestion. Liver failure means those jobs are breaking down.
The outside signs can be subtle at first. Yellow eyes, dark urine, swelling, easy bruising, itching, or tiredness may appear, but confusion, severe sleepiness, bleeding, or a possible overdose should be treated as urgent.
Frame the presentation by tempo, substrate, and synthetic function: acute liver injury, acute liver failure, decompensated cirrhosis, or acute-on-chronic liver failure. Encephalopathy plus coagulopathy in a patient without known cirrhosis should trigger ALF pathways and early transplant-center discussion.
Etiology workup and physiologic stabilization run in parallel: acetaminophen/DILI, viral hepatitis, autoimmune hepatitis, ischemic injury, vascular obstruction, pregnancy-specific disease, Wilson disease, sepsis, malignancy, and ACLF precipitants.
Patterns
Acetaminophen overdose, shock liver, severe heat injury, mushroom poisoning, and some drugs can injure many liver cells quickly.
Hepatitis A, B, or E, autoimmune hepatitis, herpes-family viruses, and idiosyncratic drug injury may present as severe acute hepatitis.
Alcohol-associated liver disease, MASH/MASLD, chronic hepatitis B or C, autoimmune disease, and inherited disorders may progress to cirrhosis.
Infection, bleeding, alcohol-associated hepatitis, portal vein thrombosis, medications, dehydration, or kidney injury can destabilize existing cirrhosis.
Cause map
The big one to know is acetaminophen, also called paracetamol. It is in many pain, fever, cold, flu, and sleep products, so people can accidentally double up. Some antibiotics, seizure medicines, bodybuilding products, herbal products, and poisonous mushrooms can also injure the liver.
Why it matters: treatment works best early. After a possible overdose, do not wait to feel sick.
Prioritize acetaminophen level and nomogram timing when possible, but treat empirically when timing is unclear and suspicion is meaningful. Look for delayed acetaminophen with falling AST/ALT but rising INR, idiosyncratic DILI, HDS injury, Amanita phalloides, cocaine/MDMA ischemic-hyperthermic injury, and mixed toxic-metabolic presentations.
Hepatitis means liver inflammation. Hepatitis A and E are often picked up from contaminated food or water. Hepatitis B can be a short infection or a lifelong one. Hepatitis C usually damages the liver slowly over years.
What doctors check: blood tests can usually tell which virus is involved and whether it is new or longstanding.
Order HAV IgM, HBsAg, anti-HBc IgM, HBV DNA when indicated, HCV antibody/RNA, and HEV testing where epidemiology or pregnancy supports it. In immunosuppressed, pregnant, or very high-aminotransferase cases, include HSV, VZV, CMV, EBV, and adenovirus; empiric acyclovir is reasonable when HSV ALF is plausible.
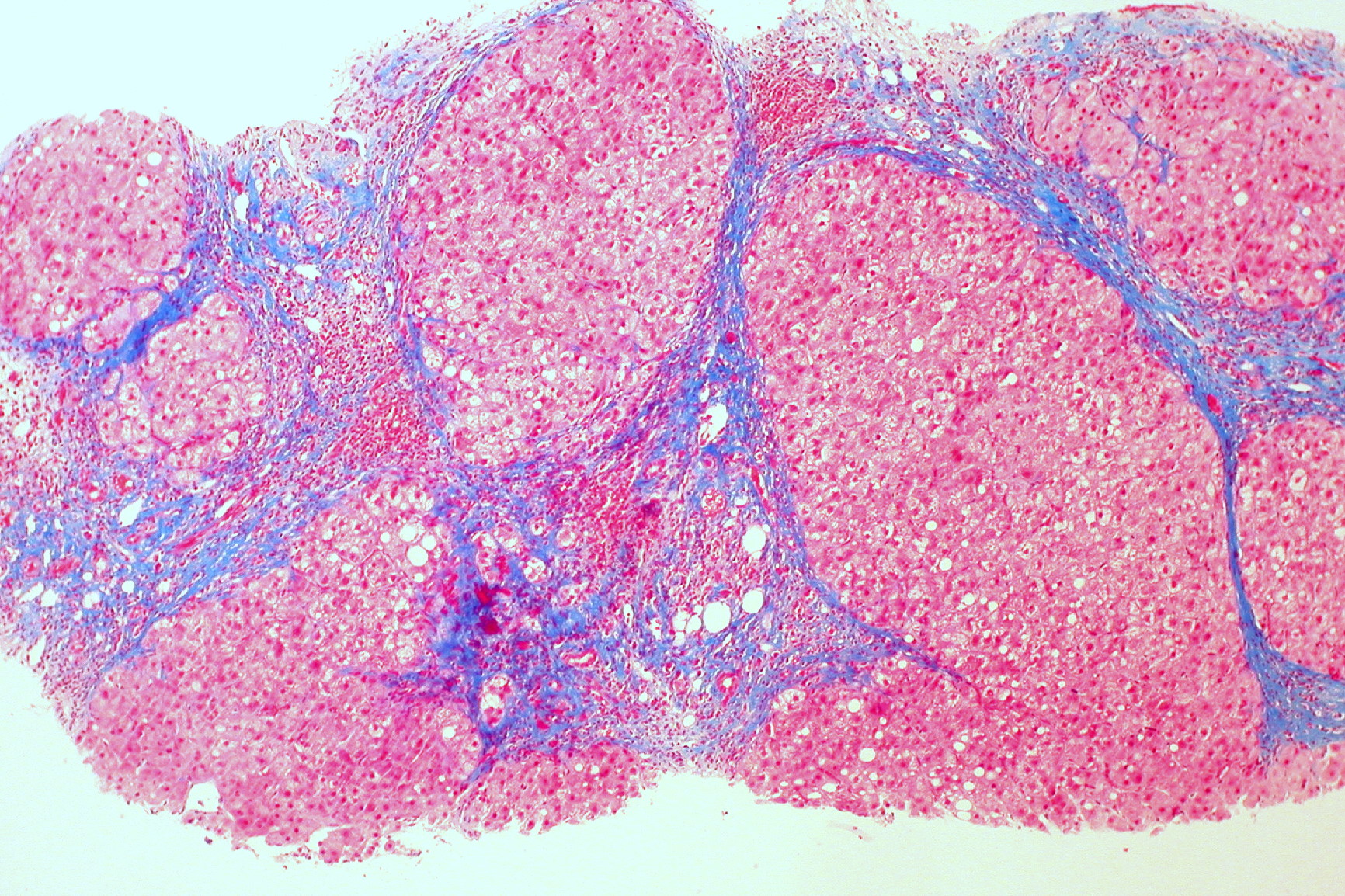
Alcohol can first cause fat to build up in the liver, then inflammation, then scar tissue. Once enough scar tissue forms, the liver may cope for a long time and then suddenly decompensate with jaundice, fluid buildup, bleeding, infection, or confusion.
Important: stopping alcohol can change the course, but withdrawal can be dangerous and may need medical supervision.
Alcohol-associated hepatitis may present as ACLF with jaundice, systemic inflammation, renal dysfunction, infection, malnutrition, and portal-hypertensive complications. Use severity tools thoughtfully, exclude infection and GI bleeding, evaluate AUD treatment needs, and consider early transplant pathways where policy and phenotype support it.
Fat can build up in the liver even in people who drink little or no alcohol. This is linked with diabetes, insulin resistance, blood pressure, cholesterol, sleep apnea, and body weight patterns. Most people do not feel it happening.
The risk: the inflammatory form, now called MASH, can quietly create scarring that later becomes cirrhosis.
Use current terminology: SLD, MASLD, MASH, MetALD, and ALD. Risk-stratify with fibrosis-focused tools rather than aminotransferase height alone. MASLD/MASH commonly coexists with cardiometabolic disease and may be the unrecognized substrate behind first decompensation.
Sometimes liver disease is not caused by alcohol, weight, or infection. The immune system can attack liver cells. Small bile tubes can become inflamed or scarred. Some people inherit problems with copper, iron, or protective proteins that slowly injure the liver.
Clue: family history, young age, other autoimmune disease, or unexplained abnormal liver tests may point doctors in this direction.
Include autoimmune hepatitis, PBC, PSC, IgG4-related cholangitis, Wilson disease, hemochromatosis, alpha-1 antitrypsin deficiency, and less common metabolic disorders. Fulminant Wilson disease remains a critical cause to identify in younger ALF patients.
The liver is full of blood vessels. If blood pressure drops very low, the heart is failing badly, or a clot blocks blood leaving or entering the liver, liver tests can worsen quickly.
Common setting: this may happen during severe infection, major bleeding, shock, advanced heart failure, or clotting disorders.
Consider ischemic hepatitis, congestive hepatopathy, Budd-Chiari syndrome, portal vein thrombosis, sinusoidal obstruction syndrome, and infiltrative vascular processes. Doppler ultrasound is an early test; CT/MRI venography, echo, thrombophilia/malignancy assessment, and hematology input may be needed.
Rare pregnancy complications can injure the liver, especially late in pregnancy or soon after delivery. Warning signs include severe right upper belly pain, headache, high blood pressure, vomiting, yellow eyes, unusual bruising, or feeling suddenly very unwell.
Do not wait: these problems need urgent obstetric and medical assessment.
Differentiate HELLP, acute fatty liver of pregnancy, severe preeclampsia, intrahepatic cholestasis, viral hepatitis, gallstone disease, and thrombotic microangiopathy. Maternal-fetal medicine and transplant/hepatology escalation should be early when synthetic dysfunction appears.
Sometimes the liver is not the first problem. A severe infection, very low blood pressure, heat stroke, or cancer spreading through the liver can overwhelm it.
Pattern: people are usually very sick overall, not just yellow or tired.
Keep malignant infiltration, lymphoma, hemophagocytic lymphohistiocytosis, septic shock, heat stroke, severe rhabdomyolysis, and multi-organ failure on the list when the liver pattern does not fit a primary hepatology diagnosis.
Safety
Liver failure can progress faster than it looks from the outside. A person can be awake and talking, then become confused or drowsy as toxins build up.
The patient-facing symptoms below map to encephalopathy, GI bleeding, portal hypertensive decompensation, cholestasis, infection, and toxic exposure. Clinical priorities are rapid triage, INR trajectory, mental status, glucose, renal function, lactate, infection search, and transfer threshold.
Workup
The liver makes proteins that help blood clot. An INR or PT test can show whether the liver is losing that ability.
Blood tests such as AST, ALT, bilirubin, and alkaline phosphatase help show whether liver cells, bile flow, or both are affected.
Doctors may check acetaminophen level, hepatitis tests, immune markers, pregnancy testing, medicine and supplement history, and inherited conditions.
Ultrasound or CT can look for blocked bile ducts, clots, swelling, scarring, or tumors. Severe cases may need a liver specialist or transplant center.
INR/PT, bilirubin, AST/ALT, alkaline phosphatase, albumin, glucose, lactate, arterial or venous blood gas, creatinine, sodium, CBC, fibrinogen when bleeding/DIC is possible, mental status grade, infection screen, and hemodynamics.
Acetaminophen level even when history is unclear, toxicology where appropriate, HAV/HBV/HCV/HEV testing, autoimmune markers and IgG, pregnancy test, HSV/CMV/EBV in selected patients, Wilson disease screen in young patients, and medication/supplement review.
Ultrasound with Doppler to assess biliary obstruction, hepatic and portal venous flow, ascites, and chronic morphology. CT or MRI is considered when vascular obstruction, malignancy, abscess, or unclear anatomy remains possible.
Early hepatology and transplant-center discussion is appropriate for ALF, worsening INR, encephalopathy, severe alcohol-associated hepatitis with organ failure, ACLF, suspected fulminant Wilson disease, and uncertain diagnosis with rapid deterioration.
Medical visuals
Sources